History of Present Illness
Medical History
Jenna's Timeline
History of Present Illness
Jenna is a 29-year-old woman who was previously diagnosed with major depressive disorder (MDD). Twelve weeks ago, she presented to her primary care physician, Dr Jones, with a chief complaint of depressed mood, diminished interest in her usual hobbies and activities, excessive sleeping, increased appetite, and weight gain. At that time, Jenna scored 19 on her Patient Health Questionnaire-9 (PHQ-9), which is suggestive of moderately severe depression, so she was diagnosed with undergoing a current major depressive episode (MDE). Jenna began pharmacotherapy with a serotonin and norepinephrine reuptake inhibitor (SNRI). After 4 weeks of initial SNRI therapy, Jenna reported mild improvements in her mood at a follow-up visit (PHQ-9 score of 16), where a dose adjustment was made. Her second follow-up at week 8 resulted in a PHQ-9 score of 14 and another SNRI dose increase. Around week 10, however, she developed sleep troubles and some irritability.
Medical History
Jenna has intermittent asthma for which she uses an inhaler. She is adherent to her combined oral contraceptive pills for birth control and the SNRI that she started 12 weeks ago. She has had 2 trials of selective serotonin reuptake inhibitors (SSRI) for MDD previously.
Jenna drinks 1 to 2 cups of coffee in the morning daily. She has 1 to 2 alcoholic beverages weekly with her partner. Jenna denies a history of smoking or other drug use.
Timeline of Jenna's Present Illness
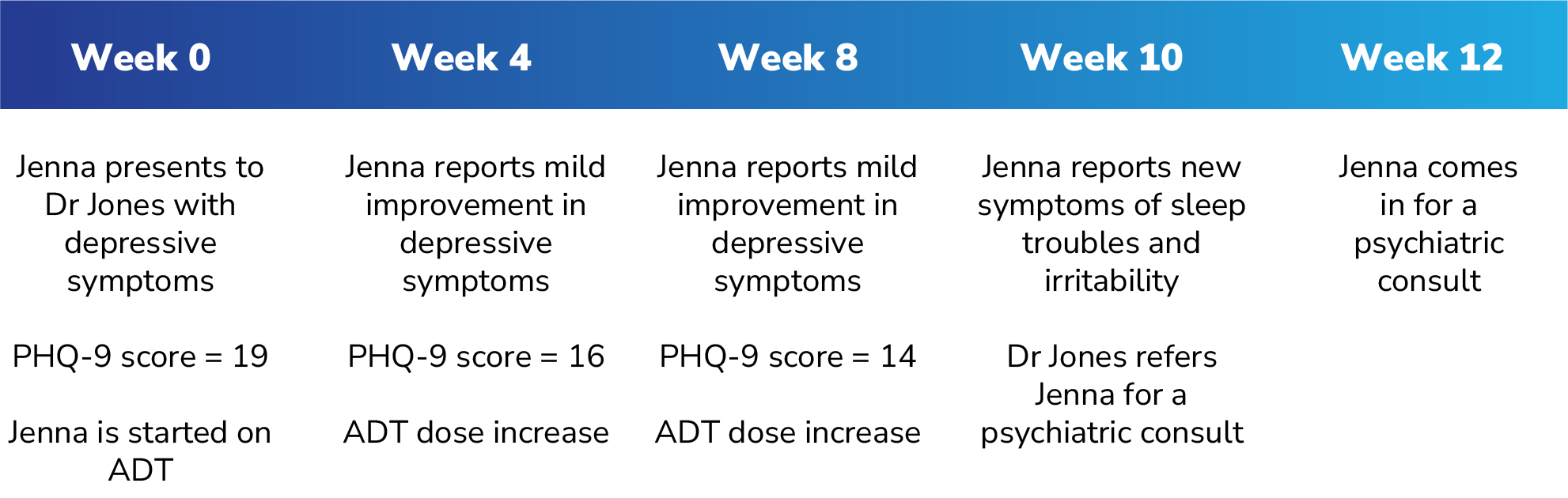
PHQ-9 = Patient Health Questionnaire-9, ADT = antidepressant therapy
Watch the video:
Screening for BP-1
Rapid Mood Screener
New Diagnosis
BP-1 Symptoms Prevalence
Screening for BP-1
During the patient interview, given his suspicions on a diagnosis other than MDD, Tony has Jenna fill out the Rapid Mood Screener (RMS), a self-administered screening tool designed to help differentiate BP-1 from MDD in patients with depressive symptoms.1
1. McIntyre RS, et al. Curr Med Res Opin. 2021;37(1):135-144.
Rapid Mood Screener
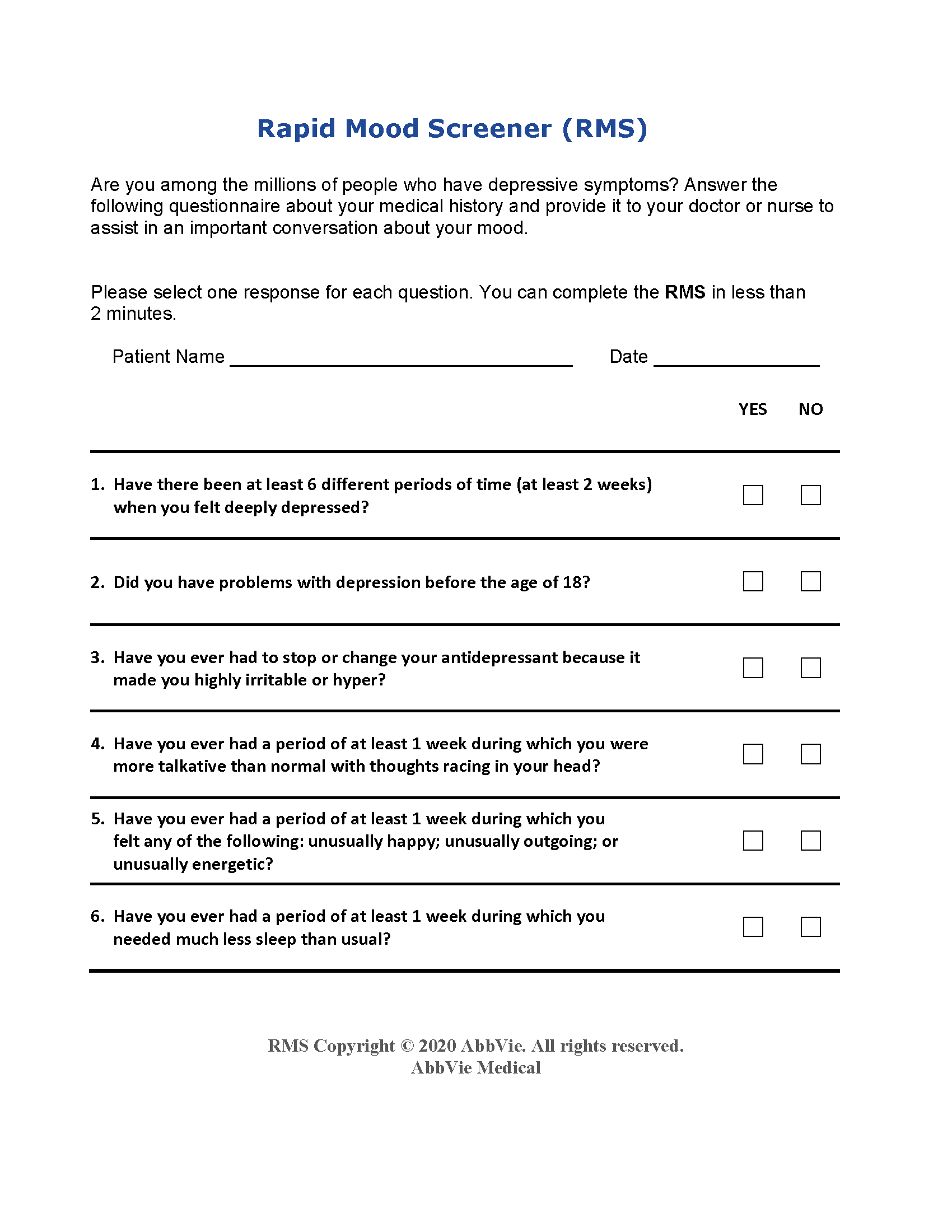
The RMS is not a diagnostic tool. The RMS tool was developed with funding and input provided by AbbVie and external experts, who received financial support from AbbVie for research, honoraria and/or consulting services depending on the author. 1. McIntyre RS, et al. Curr Med Res Opin. 2021;37(1):135-144.
New Diagnosis
Based on Jenna's and her partner's combined report, as well as her physical examination and medical history, Tony considers the shift in mood and new symptoms as potentially indicative of a different diagnosis. Jenna's response to her SNRI regimens is particularly suggestive, as patients with BP-1 who are started on an antidepressant may undergo a treatment-emergent affective switch (TEAS).
TEAS: A switch in mood polarity from depression to mania or hypomania that can be induced by certain medications, including antidepressant monotherapy1,2
1. Moller HJ, et al. Expert Rev Neurother. 2004;4(6 Suppl 2):S3-S8. 2. Salvadore G, et al. J Clin Psychiatry. 2010;71(11):1488-1501.
BP-1 Symptoms Prevalence
- Symptoms of depression in BP-1 closely resemble those in MDD.1
- Depressive symptoms are the most commonly reported symptom in patients with BP-1.2
- Patients with BP-1 may experience multiple depressive episodes in their lifetime.3
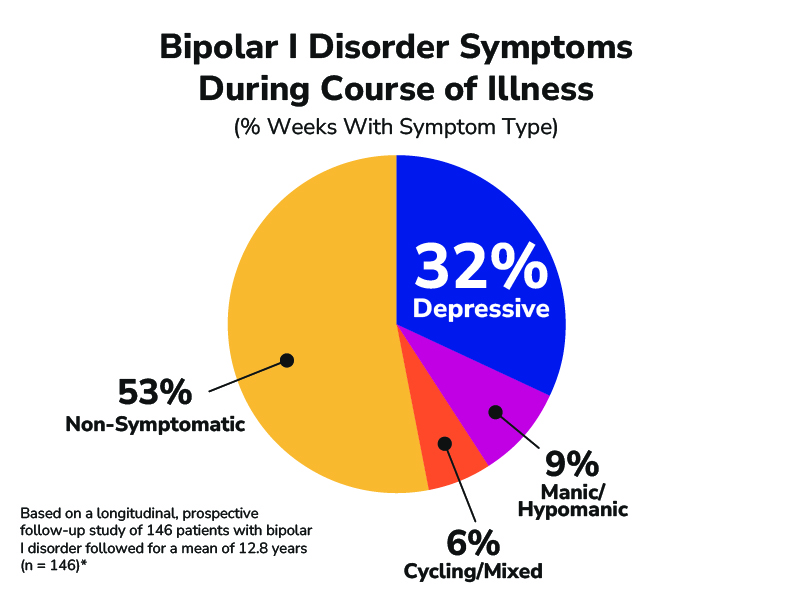
*National Institute of Mental Health Collaborative Depression Study (1978 to 1981): weekly symptom severity level based on the 6-point LIFE Psychiatric Status Rating (PSR) scale for depression and mania plus the 3-point PSR scale for rating minor depression/dysthymia, hypomania, DSM-4 atypical depression, DSM-3 adjustment disorder with depressed mood, and Research Diagnostic Criteria cyclothymic personality. 1. Culpepper L. Prim Care Companion CNS Disord. 2014;16(3):PCC.13r01609. 2. Judd LL, et al. Arch Gen Psychiatry. 2002;59:530-537. 3. Yatham LN, et al. Bipolar Disord. 2018;1-74.
Watch the video:
Alan "Tony" Amberg is a paid consultant for AbbVie Medical Affairs and was compensated for his time.

